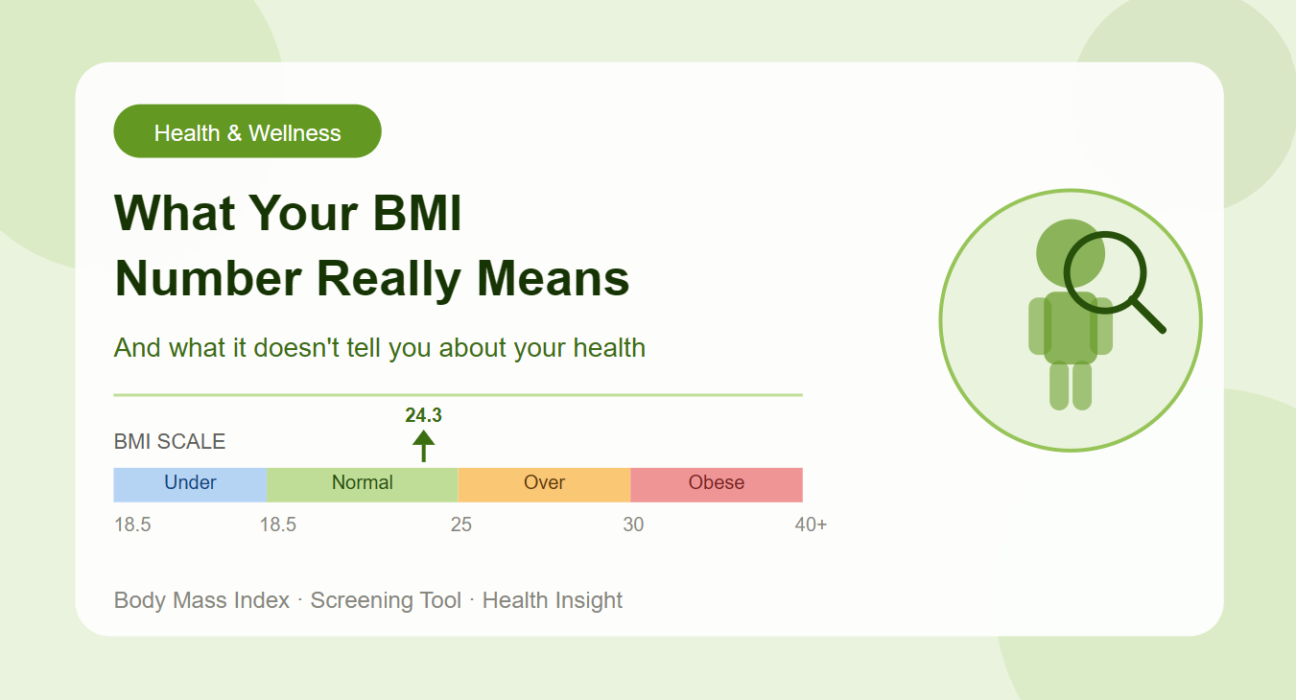
You just entered your height and weight into a BMI calculator and got a number back. Maybe it said 24.3. Maybe it said 27.8. Now what? Most people stare at that figure without knowing whether to feel relieved, concerned, or somewhere in between.
The truth is, your BMI number tells you something genuinely useful, but it does not tell you everything. Understanding both sides of that equation is what separates a panicked reaction from an informed one.
What the BMI Number Is Actually Measuring
BMI, which stands for Body Mass Index, is a ratio of your weight to your height squared. Nothing more, nothing less. It was developed in the 1830s by a Belgian mathematician named Adolphe Quetelet, not by a doctor, and was originally designed to study population trends rather than assess individual health.
When a doctor, nurse, or health app uses BMI today, they are using it as a screening tool. Think of it the way you think of a smoke alarm. It does not tell you what is on fire or how serious the situation is. It tells you that something may need a closer look.
The four standard BMI categories give you a broad signal about weight status:
A BMI below 18.5 suggests underweight status, which may point to nutritional deficiencies or underlying illness.
A BMI between 18.5 and 24.9 falls in the normal or healthy weight range, associated with the lowest population-level health risk.
A BMI between 25 and 29.9 is classified as overweight, a zone where metabolic risk begins to rise for many people.
A BMI of 30 and above is classified as obese, a range linked with significantly higher rates of heart disease, type 2 diabetes, sleep apnea, and certain cancers.
These thresholds were established using large-scale population research, which is why they carry real predictive value at the group level. For any individual, however, the picture is always more nuanced.
Where BMI Gets It Right
Despite its simplicity, BMI has earned its place in clinical practice for good reason. It is free to calculate, requires no equipment, and takes less than thirty seconds. For that reason alone, it has been validated across thousands of studies as a reasonable proxy for body fatness and associated disease risk in the general adult population.
Research consistently shows that people with higher BMI values face elevated risk of conditions including hypertension, insulin resistance, gallbladder disease, osteoarthritis, and certain hormonal cancers. At the population level, this relationship is strong enough that public health organizations worldwide, including the World Health Organization and the CDC, continue to endorse BMI as a front-line screening indicator.
For most people who are not extreme athletes and do not have unusual body composition, a BMI in the overweight or obese range is a meaningful signal that deserves attention and follow-up.
Where BMI Falls Short
Here is where the conversation gets more interesting, and more honest.
BMI measures weight relative to height. It cannot see inside your body. It has no idea whether that weight is mostly muscle, mostly fat, or somewhere in between. This creates several real blind spots.
The muscle problem. A heavily muscled person, such as a competitive weightlifter or a rugby player, may have a BMI of 28 or 29 and be classified as overweight despite having very low body fat and excellent cardiovascular health. Their weight is high because muscle is denser than fat, not because they are at elevated metabolic risk.
The fat distribution problem. Where you carry fat matters enormously for health outcomes. Fat stored around the abdomen, known as visceral fat, is far more metabolically active and dangerous than fat stored around the hips and thighs. Two people with an identical BMI of 26 may have completely different health profiles depending on their fat distribution. BMI cannot distinguish between these two scenarios at all.
The age and sex problem. Older adults tend to lose muscle mass and gain fat even when their weight stays stable. This means their BMI may remain in the normal range while their body fat percentage has climbed into a riskier zone. Similarly, women naturally carry more body fat than men at the same BMI, which means the same number can represent meaningfully different body compositions.
The ethnicity problem. Research has shown that people of Asian descent face higher metabolic risk at lower BMI thresholds compared to people of European descent. Some health organizations now recommend lower BMI cutoff points for certain Asian populations, recognizing that the standard thresholds were developed primarily from studies on white European populations.
What Doctors Actually Use Alongside BMI
Because of these limitations, BMI is rarely used in isolation by experienced clinicians. It is the starting point of a conversation, not the conclusion. Here is what typically accompanies it:
Waist circumference is one of the most important complementary measures. A waist measurement above 35 inches for women or 40 inches for men signals elevated abdominal fat and increased cardiometabolic risk, regardless of BMI.
Waist-to-hip ratio adds another layer by comparing fat around the middle to fat at the hips, giving a clearer picture of fat distribution patterns.
Body fat percentage, measured through methods such as DEXA scans, bioelectrical impedance, or skinfold calipers, directly quantifies how much of your body is fat tissue versus lean mass. This is the most direct measurement of body composition but also the most resource-intensive.
Blood panels including fasting glucose, HbA1c, lipid profile, and inflammatory markers like CRP tell the story of how your metabolism is actually functioning right now, independent of what your BMI says.
Blood pressure readings, resting heart rate, and cardiovascular fitness tests round out the picture by showing how your organs are handling the demands placed on them.
Taken together, these measures give a far more accurate and actionable health portrait than BMI alone.
How to Use Your BMI Number Wisely
Given everything above, what should you actually do with your BMI result?
If your BMI falls in the normal range, treat it as one reassuring data point, not a guarantee of perfect health. Pair it with regular check-ups, blood work, and honest attention to energy, sleep, and fitness.
If your BMI falls in the overweight range, take it seriously without catastrophizing. Check your waist circumference. Get a blood panel. Have an honest conversation with your doctor about whether your specific situation warrants lifestyle changes or monitoring.
If your BMI falls in the obese range, especially above 35, treat it as a clear signal to seek professional guidance. The associated health risks are well-documented and the earlier you engage with them, the more options you have.
If your BMI seems inconsistent with how you look and feel, because you are very muscular, very active, or have an unusual body type, ask your healthcare provider about body composition testing for a more accurate assessment.
The BMI number is not a verdict on your worth or your health. It is a starting signal. Use it as the beginning of a more complete health conversation, not the final word.
The Bottom Line
BMI is a flawed but genuinely useful tool. It gives you a fast, free, and reasonably reliable first look at whether your weight-to-height ratio falls in a range associated with good health outcomes. For the majority of adults who are not elite athletes, the BMI number carries real information worth paying attention to.
At the same time, it cannot see your muscle, your fat distribution, your fitness level, or your metabolic health. A truly complete picture of your health requires more. Think of BMI as chapter one of a longer story. It tells you where to start looking, not where the story ends.